Use the Pediatric Maintenance Fluid Calculator
Free pediatric maintenance fluid calculator using the Holliday-Segar 4-2-1 rule — get hourly IV rates and daily volumes from a child's weight in kg or lb.
Use today's actual weight — the formula tiers are based on kg
Many hospitalized children are ordered 67–80% of full maintenance
Maintenance IV rate (4-2-1 rule)
62 mL/hr
1,540 mL over 24 hours
Hourly rate (4-2-1)
62 mL/hr
Daily volume (100-50-20)
1,540 mL/day
Average intake
70 mL/kg/day
How each weight tier contributes to the hourly rate
- First 10 kg (4 mL/kg/hr · 100 mL/kg/day)10.0 kg → 40 mL/hr
- Second 10 kg (2 mL/kg/hr · 50 mL/kg/day)10.0 kg → 20 mL/hr
- Each kg above 20 (1 mL/kg/hr · 20 mL/kg/day)2.0 kg → 2 mL/hr
Quick reference: weight → full maintenance
| Weight | 4-2-1 rate | Daily volume |
|---|---|---|
| 4 kg | 16 mL/hr | 400 mL/day |
| 6 kg | 24 mL/hr | 600 mL/day |
| 8 kg | 32 mL/hr | 800 mL/day |
| 10 kg | 40 mL/hr | 1,000 mL/day |
| 12 kg | 44 mL/hr | 1,100 mL/day |
| 15 kg | 50 mL/hr | 1,250 mL/day |
| 20 kg | 60 mL/hr | 1,500 mL/day |
| 25 kg | 65 mL/hr | 1,600 mL/day |
| 30 kg | 70 mL/hr | 1,700 mL/day |
| 40 kg | 80 mL/hr | 1,900 mL/day |
| 50 kg | 90 mL/hr | 2,100 mL/day |
| 70 kg | 100 mL/hr | 2,400 mL/day |
Highlighted row = the bracket your entered weight has passed.
Your rating helps improve Pediatric Maintenance Fluid Calculator. We store only an anonymized vote (no personal data).
How to Use Pediatric Maintenance Fluid Calculator
Step 1: Enter the child’s weight
Type the current body weight in the weight field and pick kg or lb with the unit toggle — pounds are converted to kilograms automatically before the tiers are applied.
Step 2: Choose percent of maintenance
Leave the selector at 100% for full maintenance, or pick 80%, 75%, 67%, or 50% when the order calls for fluid restriction (common in bronchiolitis, meningitis, and post-op care).
Step 3: Read the hourly and daily results
The main panel shows the 4-2-1 hourly IV rate in mL/hr and the Holliday-Segar daily volume in mL/day, plus the average mL/kg/day.
Step 4: Review the tier breakdown
The stacked bar shows how the first 10 kg, second 10 kg, and remaining weight each contribute to the rate, so you can verify the math tier by tier.
Step 5: Copy the summary
Use the Copy summary button to grab weight, rate, daily volume, and any restriction percentage as plain text for notes or charting.
Key Features
- 4-2-1 rule hourly IV rate in mL/hr
- Holliday-Segar 100-50-20 daily volume in mL/day
- Weight input in kg or lb with instant conversion
- Fluid restriction presets: 80%, 75%, 67%, and 50%
- Per-tier breakdown with visual stacked bar
- Safety caps at 100 mL/hr and 2,400 mL/day
Understanding Results
The Pediatric Maintenance Fluid Calculator Formula
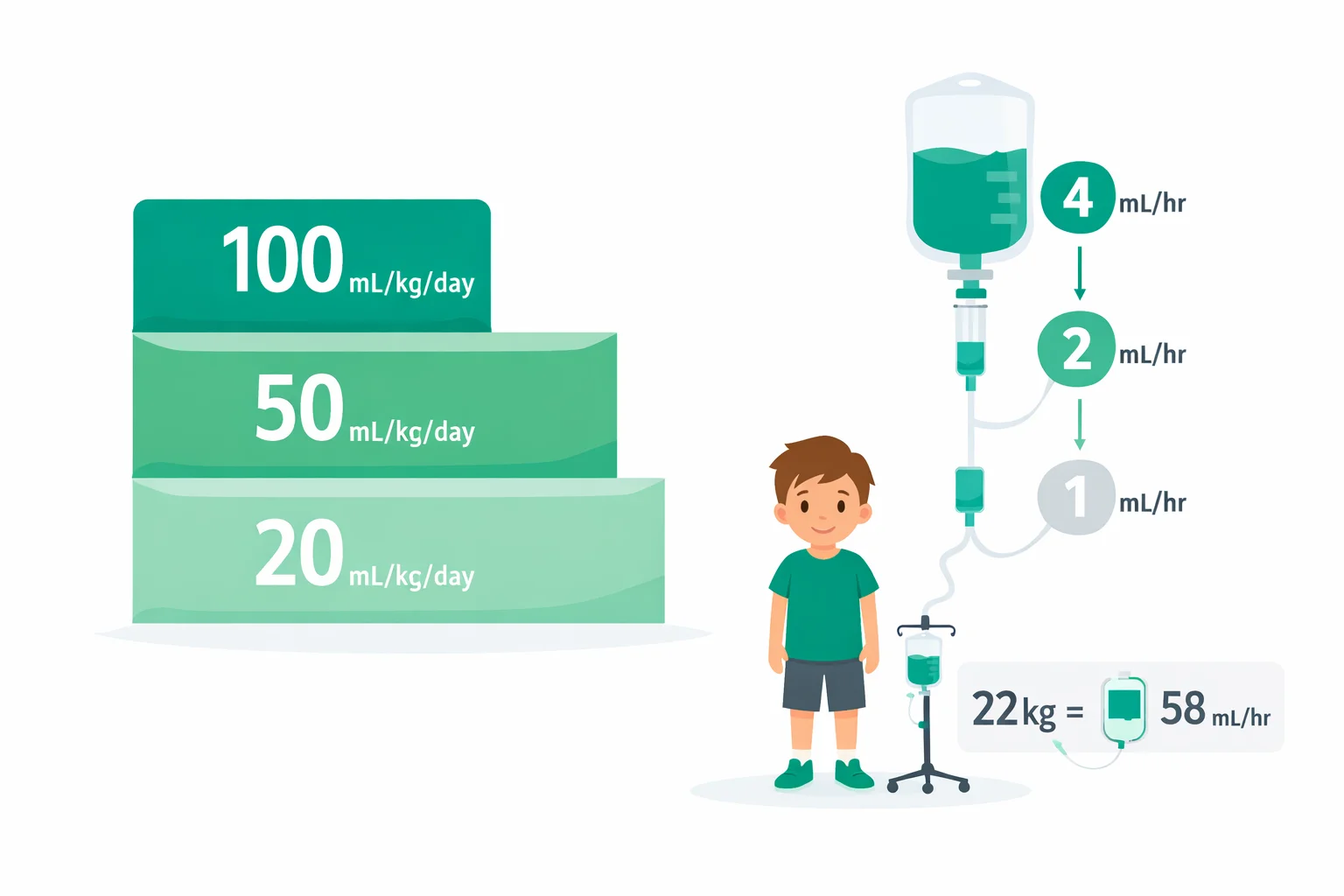
The calculator applies the Holliday-Segar method in both of its forms. Daily volume: 100 mL/kg for the first 10 kg of body weight, plus 50 mL/kg for the second 10 kg, plus 20 mL/kg for each kilogram above 20 kg. Hourly rate (the 4-2-1 rule): 4 mL/kg/hr for the first 10 kg, plus 2 mL/kg/hr for the second 10 kg, plus 1 mL/kg/hr above 20 kg. Weights entered in pounds are divided by 2.20462 first. If you select a percent of maintenance, both outputs are multiplied by that fraction (for example, 67% of 62 mL/hr = 42 mL/hr).
Reference Ranges & Interpretation
Full maintenance works out to 40 mL/hr (1,000 mL/day) at 10 kg, 60 mL/hr (1,500 mL/day) at 20 kg, 70 mL/hr (1,700 mL/day) at 30 kg, and 90 mL/hr (2,100 mL/day) at 50 kg. The calculator caps results at 100 mL/hr and 2,400 mL/day, the ceiling most institutions apply once the raw arithmetic exceeds adult volumes (above roughly 60 kg). Per the 2018 American Academy of Pediatrics guideline, the volume is usually delivered as an isotonic fluid such as dextrose 5% in 0.9% saline or lactated Ringer's for patients aged 28 days to 18 years.
Assumptions & Limitations
Holliday-Segar estimates maintenance only — it does not cover dehydration deficits, ongoing losses, or resuscitation boluses, which are calculated separately. It assumes normal renal function and normal insensible losses, so it does not apply to neonates in the first weeks of life (who are dosed by day of life starting near 60-80 mL/kg/day), and it needs adjustment for sustained fever (roughly +10-12% per degree Celsius above 38 °C), significant obesity, burns, DKA, and cardiac or renal disease. This tool is for education and cross-checking; fluid orders belong to the treating clinician.
Complete Guide: Pediatric Maintenance Fluid Calculator
A pediatric maintenance fluid calculator answers one of the most common math problems in a children's hospital: how many milliliters of IV fluid does this child need per hour? The answer almost always comes from the Holliday-Segar method, which exists in two interchangeable forms — the daily 100-50-20 version (mL/kg/day) and the hourly 4-2-1 version (mL/kg/hr). They're the same formula wearing different clothes, and knowing how they relate is the difference between a rate you can defend on rounds and a number you copied off a card. This guide walks through both forms, the 1957 physiology behind them, a fully worked 22 kg example, and the situations where the formula quietly stops being safe.
Table of contents
4-2-1 vs 100-50-20: Two Versions of the Same Formula
The daily form assigns 100 mL/kg/day to the first 10 kg of body weight, 50 mL/kg/day to the second 10 kg, and 20 mL/kg/day to every kilogram above 20. Divide those numbers by 24 and you get roughly 4.17, 2.08, and 0.83 mL/kg/hr — which someone sensibly rounded to 4, 2, and 1 for bedside use. That rounding is why the two forms disagree slightly. For a 30 kg child, 4-2-1 gives 40 + 20 + 10 = 70 mL/hr, or 1,680 mL over a day; the 100-50-20 form gives 1,000 + 500 + 200 = 1,700 mL/day, or 70.8 mL/hr. A 20 mL daily gap. Nobody cares clinically, but it confuses learners who compute both and expect identical answers.
Which one should you use? Anesthesia and emergency medicine live in mL/hr, so 4-2-1 dominates there. Ward pediatrics often writes total daily volume, especially when combining maintenance with deficit replacement. Our Holliday-Segar calculator shows both simultaneously — plus the per-tier breakdown — so the number matches however your order set is written. It doubles as a 4-2-1 rule calculator for anesthesia use and a daily-volume tool for ward orders. If you then need to convert that rate into drops per minute for a gravity set, the IV drip rate calculator handles the gtt/min conversion.
Where the Numbers Come From: A 1957 Paper on Calories
Malcolm Holliday and William Segar published the method in Pediatrics in 1957, and the logic wasn't about water at all — it was about energy. They estimated that hospitalized children expend roughly 100 kcal/kg/day for the first 10 kg of body weight, 50 kcal/kg/day for the next 10 kg, and 20 kcal/kg/day beyond that. Then they made the simplifying assumption that metabolizing each kilocalorie consumes about 1 mL of water: roughly 50 mL lost through skin and lungs (insensible losses) and 55–65 mL through urine, minus a small credit for water produced by metabolism itself.
That assumption set explains both the formula's durability and its blind spots. Energy expenditure per kilogram genuinely does fall as children grow — an infant's surface-area-to-mass ratio is far higher than a teenager's, which is why the tiers taper from 100 down to 20. But the estimates were built on healthy metabolic rates. A sedated, ventilated child in the PICU expends far less energy than Holliday and Segar assumed, which is one reason modern practice often prescribes a fraction of the calculated volume rather than the full 100%.
A 22 kg Child, Worked Both Ways
Take a 6-year-old admitted for IV antibiotics who weighs 22 kg and is NPO overnight. Hourly first:
- First 10 kg × 4 mL/kg/hr = 40 mL/hr
- Second 10 kg × 2 mL/kg/hr = 20 mL/hr
- Remaining 2 kg × 1 mL/kg/hr = 2 mL/hr
- Total: 62 mL/hr
Now daily: (10 × 100) + (10 × 50) + (2 × 20) = 1,000 + 500 + 40 = 1,540 mL/day, which works out to 64.2 mL/hr. So the pump gets programmed to 62 mL/hr under the 4-2-1 convention or 64 mL/hr under the daily convention — a 2 mL/hr difference that vanishes into the noise of a day's intake and output. What matters more is the weight itself: a weight recorded in pounds and entered as kilograms inflates the rate by a factor of 2.2, which for this child would mean running 137 mL/hr instead of 62. That's the single most dangerous error in pediatric fluid math, and it's why our calculator takes lb input directly and converts it for you — the same failure mode that makes weight-based drug dosing risky, as covered in the pediatric dose calculator.
Weight-to-Rate Reference Chart
These are full-maintenance values straight from the formula. Notice how the rate climbs steeply up to 20 kg and then flattens — above 20 kg each extra kilogram adds only 1 mL/hr.
| Weight | 4-2-1 hourly rate | 100-50-20 daily volume | Typical age |
|---|---|---|---|
| 5 kg | 20 mL/hr | 500 mL | ~2 months |
| 10 kg | 40 mL/hr | 1,000 mL | ~1 year |
| 15 kg | 50 mL/hr | 1,250 mL | ~3–4 years |
| 20 kg | 60 mL/hr | 1,500 mL | ~5–6 years |
| 30 kg | 70 mL/hr | 1,700 mL | ~9–10 years |
| 50 kg | 90 mL/hr | 2,100 mL | ~14 years |
| 70 kg | 100 mL/hr (capped) | 2,400 mL (capped) | adult-sized |
The cap matters. Run the raw arithmetic on a 90 kg adolescent and you get 130 mL/hr — 3,120 mL/day, well past anything an adult ward would order. Most institutions stop at 100 mL/hr or about 2,400 mL/day, which is where our calculator caps too. An alternative for larger or oncology patients is the body-surface-area method of 1,500–2,000 mL/m²/day; you can get the m² figure from the BSA calculator using the Mosteller formula.
Why Isotonic Fluids Won: The 2018 AAP Guideline
Holliday-Segar tells you the volume. It says nothing about what's in the bag — and that second question caused real harm for decades. The original 1957 framework paired the volume with hypotonic fluids like 0.2% or 0.45% saline, reasoning from the electrolyte content of milk. The problem: sick, post-operative, and stressed children secrete antidiuretic hormone, retain free water, and can develop hospital-acquired hyponatremia. Studies pooled for the AAP guideline found hypotonic maintenance fluids roughly doubled the risk of hyponatremia (sodium below 135 mEq/L), and severe cases caused seizures and, rarely, death.
The American Academy of Pediatrics responded with its 2018 clinical practice guideline: patients aged 28 days to 18 years should receive isotonic maintenance fluids — 0.9% saline or a balanced solution like lactated Ringer's, usually with 5% dextrose and often potassium — which cut the risk of developing a sodium below 135 mEq/L by roughly half compared with hypotonic solutions. The UK's NICE guidance reached the same conclusion in 2015. So the modern order reads something like "D5-NS + 20 mEq/L KCl at 62 mL/hr": the 62 comes from Holliday-Segar, the isotonic base comes from the 2018 guideline.
When 100% of Maintenance Is Too Much
Here's the part textbooks underplay: in many admissions, the calculated maintenance rate is a starting point that gets deliberately reduced. Any condition that raises ADH — bronchiolitis, pneumonia, meningitis, head injury, the first 24–48 hours after surgery — impairs free-water excretion, so full-volume fluids risk dilutional hyponatremia even when the fluid is isotonic. Common practice in these settings is to order two-thirds (67%) to 80% of the calculated maintenance. A 22 kg child with meningitis might therefore run at 41–50 mL/hr rather than the full 62.
Restriction goes further in oliguric renal failure, where orders may drop to insensible losses only (roughly 300–400 mL/m²/day) plus urine output replaced mL-for-mL. Heart failure patients often sit at 50–80% too. That's exactly why the calculator includes a percent-of-maintenance selector — the arithmetic of taking 67% of 62 mL/hr is trivial, but doing it mentally at 3 a.m. is how rounding errors creep into charts.
Edge Cases the Formula Misses: Neonates, Obesity, and Fever
Three groups break the model. Neonates first: the 4-2-1 rule does not apply in the first weeks of life. Term newborns start around 60–80 mL/kg/day on day 1 and step up by 10–20 mL/kg/day toward 120–150 mL/kg/day by the end of the first week, tracking the physiologic diuresis and 7–10% weight loss of the newborn period. Applying "100 mL/kg/day" to a day-1 term infant overshoots by 25–40%. Obesity second: Holliday-Segar scales with total body weight, but water needs track lean mass and metabolic rate. For a child far above the 95th BMI percentile, many clinicians calculate on an adjusted or ideal body weight to avoid overestimation, since the raw formula can exceed actual needs by 20% or more.
Fever and abnormal losses third: the formula assumes normal insensible losses. Each 1 °C of sustained fever above 38 °C adds roughly 10–12% to water needs; radiant warmers, phototherapy, tachypnea, burns, and high-output stomas all add more. The reverse applies to mechanically ventilated patients breathing humidified gas, whose respiratory losses approach zero. None of that lives inside the formula — it lives in the reassessment. Weigh daily, track ins and outs, check electrolytes within 24 hours of starting IV fluids, and treat the calculated number as the anchor you adjust from, not a set-and-forget rate.
References
- Holliday MA, Segar WE. The maintenance need for water in parenteral fluid therapy. Pediatrics. 1957;19(5):823–832. PubMed
- Feld LG, Neuspiel DR, Foster BA, et al. Clinical Practice Guideline: Maintenance Intravenous Fluids in Children. Pediatrics. 2018;142(6):e20183083. AAP Publications
- National Institute for Health and Care Excellence. IV fluid therapy in children and young people in hospital (NG29). 2015, updated 2020. NICE

Written by Jurica Šinko
Founder & CEO
Entrepreneur and health information advocate, passionate about making health calculations accessible to everyone through intuitive digital tools.
View full profileFrequently Asked Questions
What is the 4-2-1 rule for pediatric maintenance fluids?
The 4-2-1 rule assigns 4 mL/kg/hr for the first 10 kg of body weight, 2 mL/kg/hr for the second 10 kg, and 1 mL/kg/hr for every kilogram above 20 kg. It is the hourly form of the Holliday-Segar method. For a 25 kg child that works out to 40 + 20 + 5 = 65 mL/hr.
How much maintenance fluid does a 22 kg child need?
A 22 kg child needs 62 mL/hr by the 4-2-1 rule (40 + 20 + 2) or 1,540 mL/day by the daily 100-50-20 form (1,000 + 500 + 40). Those two answers differ by about 2 mL/hr because 4-2-1 rounds the per-hour rates, and either is acceptable in practice.
Why do the 4-2-1 rate and the daily Holliday-Segar volume not match exactly?
Dividing 100, 50, and 20 mL/kg/day by 24 gives 4.17, 2.08, and 0.83 mL/kg/hr, which were rounded to 4, 2, and 1 for bedside use. For a 30 kg child the daily form gives 1,700 mL (70.8 mL/hr) while 4-2-1 gives 70 mL/hr — a roughly 1-3% difference that is clinically insignificant.
What IV fluid does the AAP recommend for maintenance in children?
The 2018 AAP clinical practice guideline recommends isotonic fluids — 0.9% saline or a balanced solution like lactated Ringer’s, usually with 5% dextrose — for patients aged 28 days to 18 years. Isotonic solutions roughly halve the risk of hospital-acquired hyponatremia (sodium below 135 mEq/L) compared with hypotonic fluids.
When should a child get less than 100% of calculated maintenance?
Conditions that raise antidiuretic hormone — bronchiolitis, pneumonia, meningitis, head injury, and the first 24-48 hours after surgery — impair free-water excretion, so many teams order 67-80% of the calculated rate. Oliguric renal failure and heart failure may be restricted further, sometimes to insensible losses plus urine output.
Does the Holliday-Segar formula work for newborns?
No. In the first weeks of life fluids are prescribed by day of life: term newborns typically start at 60-80 mL/kg/day on day 1 and advance by 10-20 mL/kg/day toward 120-150 mL/kg/day by the end of the first week. Applying 100 mL/kg/day to a day-1 infant overshoots by 25-40%.
What is the maximum pediatric maintenance fluid rate?
Most institutions cap the rate at about 100 mL/hr, or roughly 2,400 mL/day, which the raw formula exceeds above 60 kg. For larger patients or oncology protocols, the body-surface-area method of 1,500-2,000 mL/m2/day is a common alternative.
Should I use actual or ideal body weight for maintenance fluids in an obese child?
Many clinicians use ideal or adjusted body weight, because water needs track lean mass rather than total mass. Running the formula on actual weight in significant obesity can overestimate needs by 20% or more, increasing the risk of fluid overload and hyponatremia.
Related Calculators
Apgar Score Calculator — Newborn Health at 1 & 5 Minutes
Use the Apgar score calculator to rate a newborn at 1 and 5 minutes across heart rate, breathing, muscle tone, reflexes, and skin color on a 0 to 10 scale.

Baby Food Calculator — Solids Introduction & Portions
Estimate age‑appropriate portions and plan meal frequency with the baby food calculator. Log new foods, track allergens, and export a simple weekly menu.

Infant Growth Chart Calculator
Track weight, length, and head size with the infant growth chart calculator using WHO percentiles. See trends on clear charts and compare age-based progress.

Baby Length Percentile Calculator — WHO Reference Guide
Check WHO length‑for‑age percentiles with the baby length percentile calculator. Input age, sex, and length to see your percentile and track growth trends.

Baby Milestone Calculator — Track Skills by Age & Stage
Use our baby milestone calculator to see what’s typical by corrected age. Explore early, typical, and later windows for motor, language, and cognitive skills.

Baby Weight Percentile Calculator — WHO Growth Guide
Use the baby weight percentile calculator to see WHO weight‑for‑age percentiles. Enter age, sex, and weight to get your percentile, z‑score, and tips.